Fieldwork: Observing Dialysis in Utrecht
In my last post I alluded to finished fieldwork at the dialysis ward of UMC Utrecht. Now, I’d like to share more about what I did and found out!
As a background, I visited UMCU in February-March for a total of ten shifts over three weeks. Plan A here was to finish observations in two weeks, but I quickly noticed that a full day of observations is exhausting, and learned to sprinkle recovery days between observations.
As I understand it, when people are put into a new context we quickly come up with simplifying heuristics to get some bits of our being into autopilot. Making simplifications about how to act and talk, who is “in” and who is “out”, what to pay attention to and what to ignore saves up processing power and lets you quickly tell yourself that you understand.
This is of course, unfortunately, the opposite of what I was going for with this fieldwork. I like the expression that sociology involves seeing the familiar as strange, and I tried to intentionally hold onto the strangeness of everything for as long as I could, and write it into my notes. I also stand behind what I said to the dialysis crew upon our first meeting: If I judge anyone I’m observing, I will have failed at my job. Quick moral judgements are unhelpful to begin with, but in trying to understand why things happen, they block access to complexity and ruin the whole exercise.
Being a person though, I of course failed and did make quick judgements and simplifications and all of it, but hopefully less than if I hadn’t struggled against them.

The UMC Utrecht concorde. As for many, this was my first introduction to UMCU and to working in a hospital. This is where I processed my relationship with hospitals and the weird gliding past of patient and professional lives. For some, the few hours that they spend here become long-told stories about profound questions of life and death. For some, it’s Tuesday.
There were some conversations beforehand on whether I should wear the hospital whites or not. On one hand, they mark someone who can help a patient in need (which I can’t), and on the other someone who is a legitimate, trustworthy part of the hospital environment. You see we focused on the latter - if anyone came to me for help, I could always redirect them to a nearby nurse.
What is Dialysis?
Dialysis is a life-sustaining treatment for when your kidneys are barely functioning. It temporarily replaces kidney functioning by taking excess water and metabolic waste out of your body - something that would normally be done through peeing.
The two main types of dialysis are
Hemodialysis, where blood (“hemo”) is pumped out of the body to go through a filter and back. This is done at dialysis centers or hospitals, and is the focus of my work.
Peritoneal dialysis, where fluid is pumped to the abdominal cavity, where it takes on the undesired substances via osmosis. This can be done at home, and was not a part of my observations.
For patients, hemodialysis is not only life sustaining but also life changing. The average hemodialysis (from hereon just dialysis) patient receives treatment three times a week for about 4 hours at a time. Add to that the travel time, the time spent recovering from the unpleasant sensations of a “dialysis hangover” some experience and the attention you need to pay to e.g. your water intake between sessions. Dialysis, helpful as it is, takes over a patients life to an extent. Luckily many also find community in the group of people they meet at these frequent dialysis sessions and make even friends.
For nurses, and dialysis is heavily led by nurses, dialysis is one of the few wards where you can actually get to know your patients as they come back time and time again. At UMCU dialysis nursing is also highly appreciated and autonomous, and the nurse-led treatments in my view lower the hierarchical distance between nurses and doctors somewhat. As mostly non-acute care, dialysis also has no night shifts, which I am told is an attractive marketing hook for those emphasizing work-life balance.
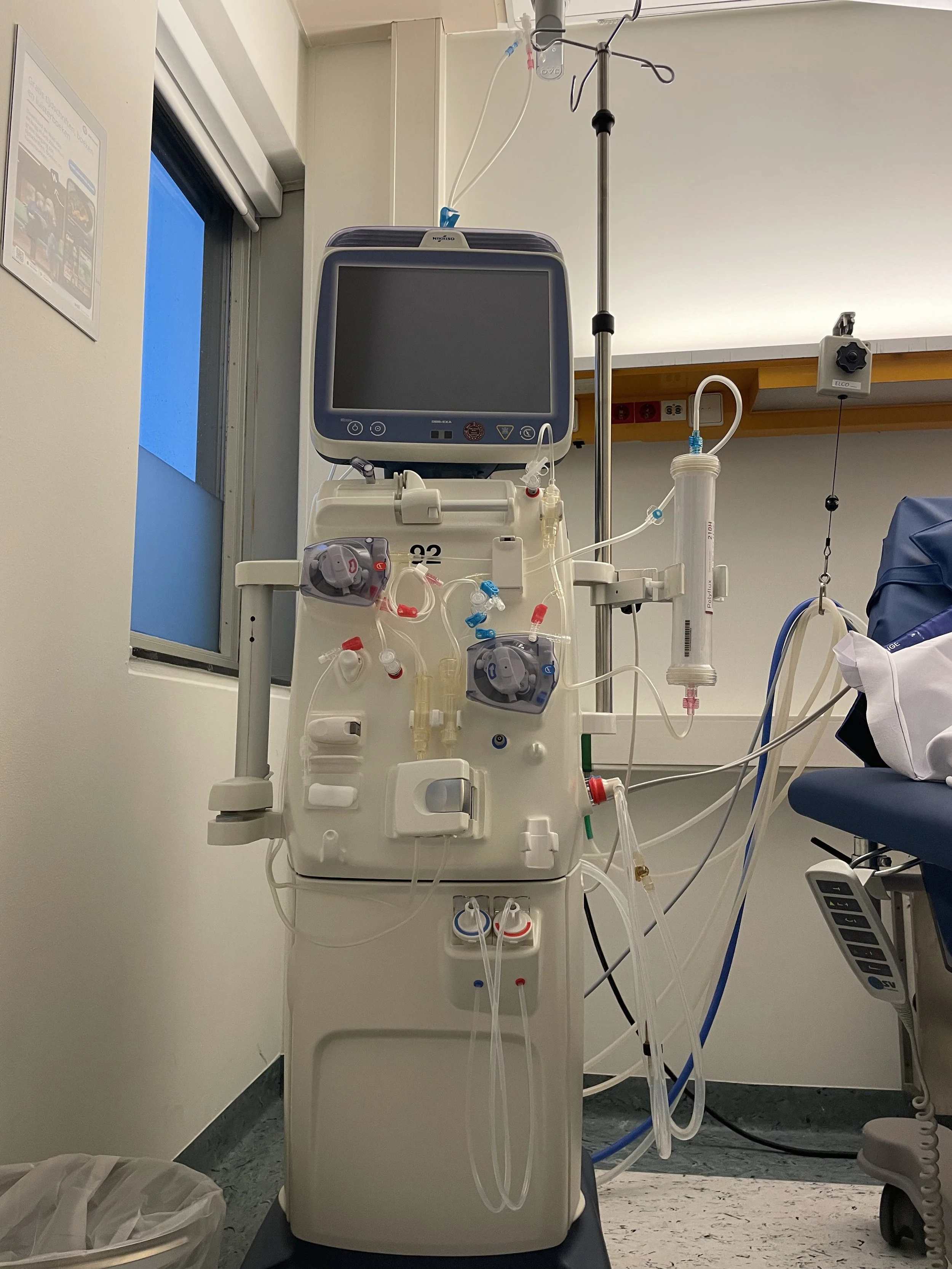
A dialysis machine from the UMCU fleet. This is a specific model, but shows you the many tubes (blood lines) that blood travels through to go into the filter (artificial kidney) on the right and back. The machine is pretty talkative, and will beep when unhappy, give next steps for prep and cleanup, and display time left and other stats during the treatment.

I’m still uneasy about using a camera at the ward. I think it made others uneasy too, so even though I could have asked for permission to photograph the staff, I mostly stuck to empty treatment rooms and inanimate objects. At least the light was nice.
What did I do?
My methodology is something called “focused ethnography”, which is a little like how you’d imagine traditional anthropology but make it more limited in time and scope. Essentially you immerse yourself into a new cultural context and note your observations, in my case into notebooks and voice recordings.
One of my main takeaways for future fieldwork was on these different kinds of notes. For one, I was surprised that I was allowed to photograph non-patient scenes, which was immensely helpful. Second, I learned that while written notes are great for quietly recording events going outside of me, writing detailed notes in the middle of a rich conversation ruins said conversation. This is why I quickly switched to just focusing on the conversation while in it and then right after scurrying to a hallway or an empty room to repeat it and my initial impressions to a voice recorder.
I was also surprised and a little humbled how much easier it was to take these notes in Finnish rather than English. Do not underestimate the power of the mother tongue - cognition connection.

The winter olympics were on during my observation period, so of course the whole ward - patients and nurses - had to tune in to watch team Oranje skating 😎
What did I learn?
So much, but to pick three of my favorite points:
Just how strong the medical ideals are, of the primacy of human life and of medico-scientific knowledge. In rest of society we tend to be pretty post-modern, not really orienting ourselves around grand narratives or moral principles. At the same time trust in institutions like science and medicine is falling among the general public, but within those institutions there’s meaning and direction like I’ve never seen before.
Long-term leadership focus on sustainability can have an impact. UMC Utrecht and the dialysis ward are at the forefront of green dialysis efforts and that’s not only because of extraordinary individuals or sufficient resources to allow mental capacity for secondary priorities, but also because long-term emphasis on sustainability e.g. has brought in EU-funding for projects, normalized sustainability as a part of working there and attracted dedicated individuals who increase the impact even further.
That, at least in this case, the materials are the treatment. Dialysis as a treatment is technological, and as such, reaching the level of change required for circularity has to center the product manufacturers. Combining the high-tech design of medical products with the protocolized nature of work creates a strong “one right way” of doing things that is best changed (collaboratively) from the product side up.
Now off to new adventures with obstetrics in Rotterdam!