“Why is dialysis the way it is?” - a living lab discussion
Quick update from the UMC Utrecht living lab!
In the ESCH-R project we have two permanent “living labs”, one in Rotterdam and another in Utrecht. Those of us who do research at UMC Utrecht meet there about every two weeks to share results and perspectives.
Last Friday I was booked to lead a session and share my recent observations from the dialysis ward. In February-March I spent 10 shifts over 3 weeks observing how dialysis is done at the UMC Utrecht, looking for connections between single-use products and the other aspects of work in play there.
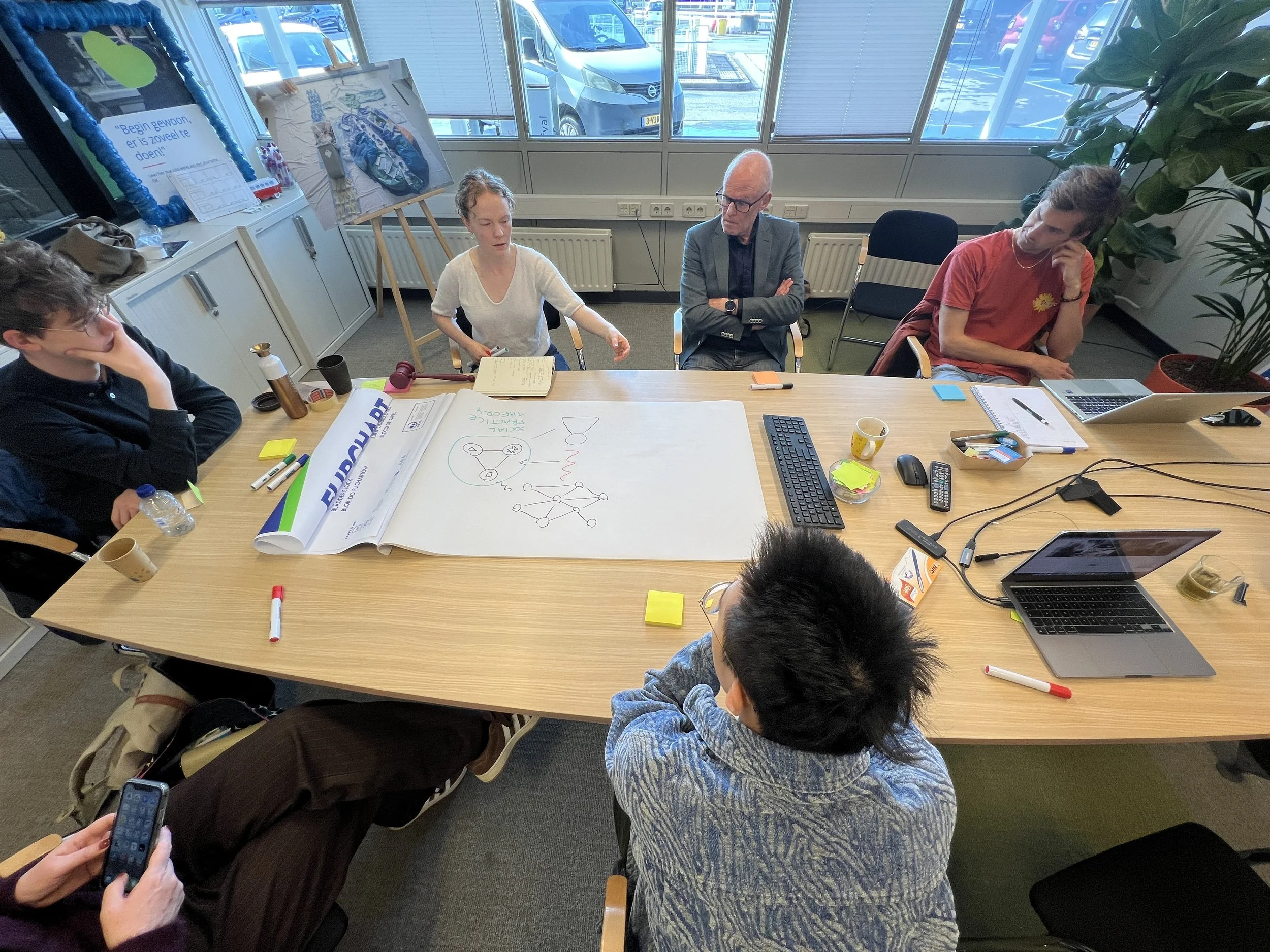
Talking and drawing our way through how social practices sit between approaches focused on agency (individuals) or structure (systems).
I opened with a quick overview of how my approach, social practice theory, differs from the more dominant views of seeing how society works. Although a colleague had named the session “Heidi’s take on behavior” (😅) I don’t work on behavior, that would be taking an individualist lens on social life. I also don’t work on broad systems or structures, although they inform my work and set a context for it. What I look at are social practices, i.e. shared patterns of routinized activity that could be seen as connecting individuals with those broad structures of society.
It was great and frankly surprising how interested and engaged my colleagues from various different fields were with social theory! I had expected the theory bit to be almost a necessary evil, but there was quite some interest in learning to see the world from a new angle, or maybe just in the work of a colleague. Either way, what a priviledge!
Then we explored our perceptions of why dialysis is the way it is. I started talking through my observations at the dialysis ward while drawing the main elements and influencing factors for a practice:
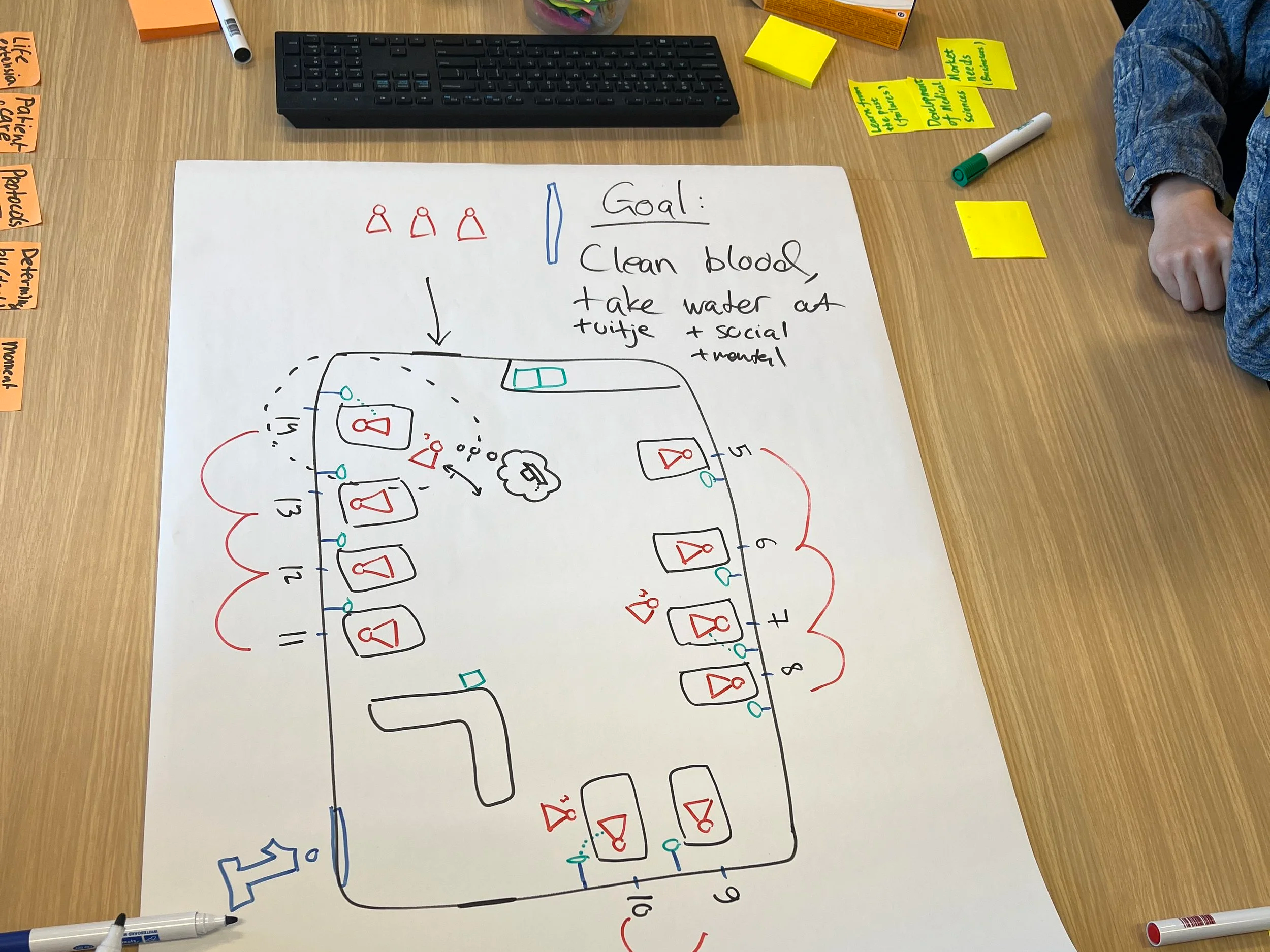
All practices have a goal or a project that gives it a reason for being. Discussing the many goals associated with dialysis already brought in a lot of helpful complexity in understanding the rest of the practice.
There’s a space: a dialysis ward, with a particular shape and location. There’s architectural history that influences how dialysis is given, and how patients experience their treatment.
There is time, in multiple ways: dialysis at UMCU happens in two shifts, within which there is a tempo and a rhythm. Each dialysis treatment has its own time, connected to the metabolism and other biological processes (time dimension!) within the patient body. Patients and providers are acutely aware of the time dialysis takes up in the patient’s life and do their best to limit it.
There are materials: dialysis machine, blood lines, needles, wrappings, chairs and beds create the immediate physical context of dialysis. There is a dizzying array of specially designed objects ranging from infrastructural (ultrapure water, dialysate, electrical and data systems) to daily tech (nurse computers, dialysis machines) to disposables. Each of these has been designed for a specific way of use, some in specific moments of the treatment.
There are norms and values, most importantly the primacy of human life.
And among many other aspects, there are the practictioners (mainly patients and nurses), competences from training and experience, and many connected practices such as those of procurement, waste management and professional management.
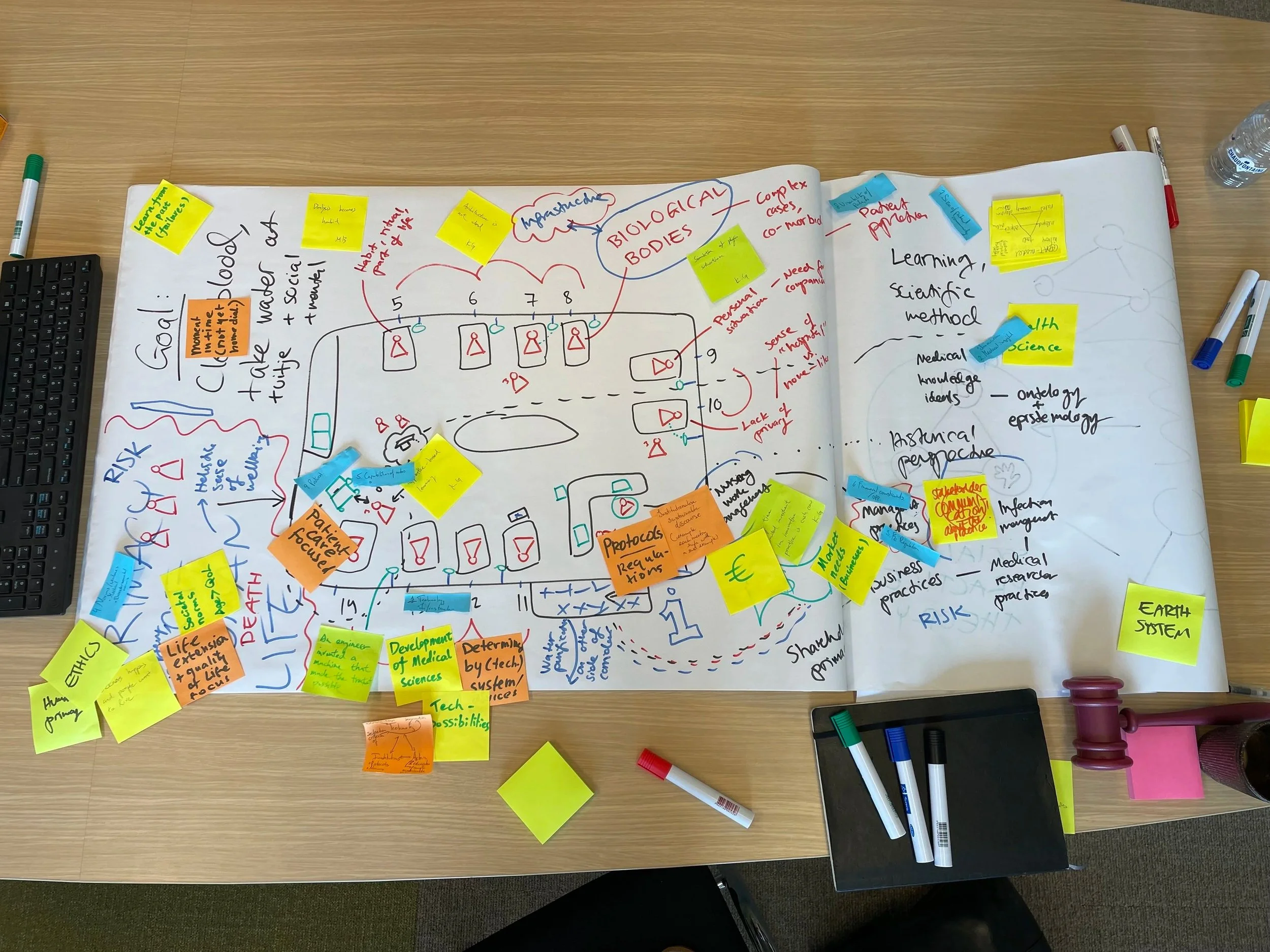
A visual exploration of “why dialysis is the way it is”
So by discussing these elements, what did we find? To summarize the conversation into three points:
Historicity. These elements have co-evolved with each other and other practices for decades, and this creates system lock-ins. Learning how the current elements and connections came to be would be a powerful force for recognizing and changing that which we would no longer conciously choose.
Everything is connected, but some connections matter more than others. Societal norms on life and death, hospital architecture and nursing team dynamics all influence how dialysis is given, but for circular economy it is clear practices of product design, maufacturing and procurement have the most direct influence on the material footprint of dialysis.
Medical norms and ideals are alive and well, and this centrality of ideals differentiates healthcare from most other sectors. Though hospitals do have profit incentives and include business logics in their operations, unnecessary cynisism on why hospitals work the way they do would obscure a major dimension of why hospital work is the way it is.